Asphalt paving for medical and high-traffic facilities is a specialized discipline that balances heavy structural demands, strict regulatory compliance, and uninterrupted facility operations. We built this guide around pavement engineering and design, ADA compliance and parking layout, drainage and climate resilience, phased construction logistics, and long-term maintenance planning.
Pavement engineering for these facilities starts with the loads emergency vehicles impose. Ambulances and fire trucks carry axle weights ten or more times greater than passenger cars, requiring thicker asphalt sections, reinforced aggregate bases, and carefully prepared subgrades. Mix designs like Stone Matrix Asphalt use stone-on-stone contact to resist rutting in stop-and-go zones where standard mixes would deform.
ADA compliance and parking layout drive much of the design geometry. Medical facilities must meet elevated accessible parking ratios, strict slope tolerances on pedestrian routes, and surface texture standards that balance wheelchair rollability with slip resistance. Emergency vehicle lanes, patient drop-off zones, and wayfinding striping all layer onto these requirements.
Drainage and climate resilience protect the investment over time. Proper surface grading, strategically placed catch basins, and slope design channel water away from building entries and heavy-load zones. In Colorado, freeze-thaw cycles, aggressive deicer use, and UV radiation nearly twice as intense as sea level accelerate pavement aging and cracking.
Phased construction keeps facilities operational throughout paving projects. Staged work zones, night paving schedules, and coordinated traffic control maintain emergency access and patient safety without shutting down critical areas.
Ongoing maintenance, including sealcoating, annual crack sealing, and informed overlay decisions, extends pavement life and prevents the structural failures that force costly full-depth replacements.
Why Do Medical and High-Traffic Facilities Have Unique Paving Requirements?
Medical and high-traffic facilities have unique paving requirements because they must support heavy emergency vehicles, meet strict accessibility standards, and maintain uninterrupted access around the clock. The sections below cover traffic loads, emergency vehicle design impacts, and scheduling challenges.
What Traffic Loads Must Medical Facility Pavements Withstand?
Medical facility pavements must withstand significantly heavier and more frequent traffic loads than standard commercial lots. Ambulances, fire trucks, supply delivery vehicles, and patient transport vans impose concentrated axle weights that exceed typical passenger car loads by a factor of ten or more. These heavy vehicles follow repetitive routes to emergency entrances, ambulance bays, and loading docks, compounding stress on specific pavement sections.
Standard parking lot asphalt designs often fail prematurely under this kind of sustained, channelized heavy loading. For medical facilities, pavement engineers must account for both the weight and the frequency of these loads when specifying thickness and base layers. Ignoring either factor leads to rutting, fatigue cracking, and costly early replacement.
How Do Emergency Vehicle Access Needs Affect Pavement Design?
Emergency vehicle access needs affect pavement design by imposing stricter structural, dimensional, and clearance requirements than standard commercial projects demand. Under the FAST Act, emergency vehicles are permitted axle weights up to 24,000 pounds on a single steering axle and 62,000 pounds on a tandem axle, according to the Federal Highway Administration. These loads require thicker asphalt sections with reinforced base courses.
Dimensional standards add further constraints. Fire department access roads must maintain:
- A minimum unobstructed width of 20 feet.
- An unobstructed vertical clearance of 13.5 feet.
Turning radii at intersections and entry points must also accommodate ladder trucks and heavy rescue apparatus. Pavement designs that fail to account for these combined weight and geometry requirements risk structural failure in the zones where reliable access matters most.
Why Does 24/7 Operations Scheduling Complicate Paving Projects?
24/7 operations scheduling complicates paving projects because medical facilities cannot shut down parking areas, access roads, or emergency entrances for extended periods without jeopardizing patient safety. Every lane closure must be carefully coordinated with hospital administration, emergency services, and traffic management teams.
Phased construction offers a practical solution. This approach isolates renovation areas to minimize noise and dust that could affect patient safety while maintaining continuous emergency access. Work windows often shrink to overnight or weekend shifts, which limits the volume of asphalt that can be placed and compacted before the area must reopen. Curing times, equipment staging, and material deliveries all need adjustment.
This operational reality is why experienced paving contractors who understand healthcare logistics deliver better outcomes than general paving crews unfamiliar with these constraints.
What Pavement Design Factors Matter Most for Medical Facilities?
The pavement design factors that matter most for medical facilities include pavement thickness, base layer composition, subgrade preparation, and asphalt mix design. Each factor addresses specific structural demands unique to healthcare environments.
How Should Pavement Thickness Be Specified for Ambulance Bays?
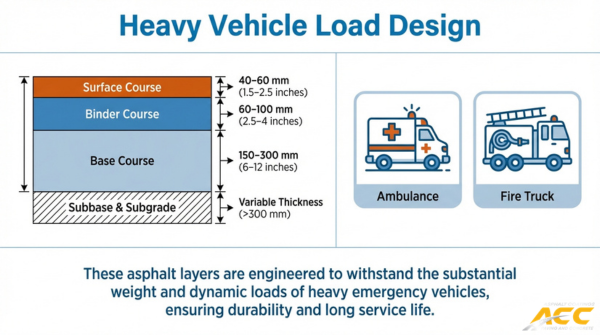
Pavement thickness for ambulance bays should be specified based on expected axle loads and vehicle dwell times. Ambulances and heavy emergency apparatus exert concentrated forces, especially when idling or parked for extended periods at loading zones.
A minimum full-depth asphalt section of 6 to 8 inches is common for ambulance bays, though site-specific engineering analysis may call for greater thickness. The surface course, binder course, and base course each serve a distinct structural role:
- The surface course resists tire wear and weather exposure.
- The binder course distributes loads across a wider area.
- The base course transfers stress into the underlying aggregate and subgrade.
Thinner sections risk premature fatigue cracking under repetitive heavy loading, making conservative thickness specifications a practical safeguard for facilities that cannot afford unplanned closures.
What Base Layer Requirements Apply to High-Traffic Entry Lanes?
The base layer requirements for high-traffic entry lanes center on load distribution and long-term stability. Entry lanes at medical facilities absorb constant turning, braking, and acceleration from patient vehicles, delivery trucks, and emergency transports simultaneously.
Crushed aggregate base material should meet strict gradation standards to lock particles together and resist shifting under repeated stress. Key requirements include:
- A minimum compacted aggregate base depth of 8 to 12 inches for heavy commercial traffic.
- Proper gradation with angular, fractured stone to maximize interlock.
- Adequate compaction to 95% or greater of maximum dry density.
Without a properly engineered base, even well-designed surface courses will crack and deform prematurely. Base failure is one of the most common causes of early pavement distress in high-traffic commercial lots.
How Does Subgrade Preparation Differ for Heavy-Load Zones?
Subgrade preparation for heavy-load zones differs by requiring more rigorous evaluation, deeper treatment, and stricter compaction standards than standard parking areas. The subgrade is the native soil beneath the aggregate base, and its bearing capacity determines how much load the entire pavement structure can support.
Heavy-load zones, such as ambulance bays, loading docks, and dumpster pads, demand thorough geotechnical testing to identify weak or expansive soils. Preparation typically involves:
- Proof-rolling to detect soft spots before placing aggregate.
- Over-excavation and replacement of unsuitable soils with engineered fill.
- Chemical stabilization with lime or cement for clay-heavy subgrades.
- Compaction testing at multiple lifts to verify uniform density.
Skipping these steps in heavy-load zones often leads to differential settlement, which causes surface cracking and ponding water.
What Mix Design Properties Resist Rutting in Stop-and-Go Areas?
The mix design properties that resist rutting in stop-and-go areas are aggregate structure, binder stiffness, and volumetric composition. Rutting occurs when asphalt deforms under sustained or repeated tire pressure, a problem especially pronounced where vehicles brake, idle, and accelerate at facility entrances, drive-throughs, and drop-off zones.
According to the National Asphalt Pavement Association, Stone Matrix Asphalt relies on stone-on-stone contact for structural strength and a rich mortar binder for durability, producing a tough, rut-resistant mixture suited to high-traffic environments. Beyond SMA, several properties contribute to rut resistance:
- High-quality, cubical aggregates that interlock under compaction.
- Polymer-modified binders that maintain stiffness at elevated pavement temperatures.
- Low air void content to limit post-construction densification under traffic.
Facilities in regions with frequent freeze-thaw cycles also need mix designs that balance rut resistance with cracking flexibility, since overly stiff mixes can become brittle in cold weather. Selecting the right mix requires balancing these competing demands against each facility’s specific traffic patterns.
With structural design addressed, ADA compliance requirements add another critical layer to medical facility paving.
How Do ADA Compliance Requirements Shape Facility Paving?
ADA compliance requirements shape facility paving by dictating precise slope tolerances, accessible parking ratios, pedestrian route standards, and surface textures. The sections below cover slope and grade standards, crosswalk and pedestrian route paving, and surface texture requirements for wheelchair access.
What Slope and Grade Standards Apply to Accessible Parking Areas?
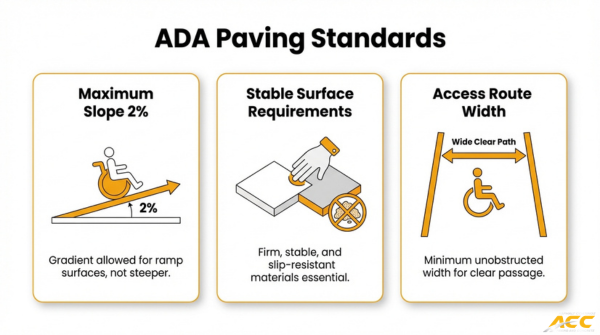
The slope and grade standards that apply to accessible parking areas are defined by the U.S. Access Board and ADA guidelines. Accessible parking surfaces must remain as flat as possible while still allowing drainage. According to the U.S. Access Board, portions of accessible routes with running slopes steeper than 5% must be treated as ramps, which are limited to a maximum running slope of 1:12 (8.33%) and a maximum cross slope of 1:48 (2.08%).
Medical facilities face stricter accessible parking quantity requirements as well. Hospital outpatient facilities must designate ten percent of patient and visitor parking as accessible, while rehabilitation and outpatient physical therapy facilities require twenty percent. Achieving these ratios while maintaining proper grade tolerances demands careful grading during asphalt installation, particularly on sloped sites where drainage needs compete with accessibility standards.
How Must Crosswalks and Pedestrian Routes Be Paved for Compliance?
Crosswalks and pedestrian routes must be paved with smooth, stable, and firm surfaces that provide a continuous accessible path of travel. ADA standards require that pedestrian routes maintain consistent grade without abrupt level changes exceeding a quarter inch. Joints, cracks, and surface irregularities along these paths can catch wheelchair casters or create trip hazards for patients using mobility aids.
Proper asphalt compaction is essential in these zones. Poorly compacted crosswalk surfaces settle unevenly over time, creating the exact level changes that violate accessibility standards. Detectable warning surfaces, typically truncated dome mats, must also be installed at curb ramps where pedestrian routes meet vehicular traffic. For medical facilities with high foot traffic, these elements require precise installation to remain both functional and compliant over years of heavy use.
What Surface Texture Requirements Ensure Safe Wheelchair Access?
The surface texture requirements that ensure safe wheelchair access balance traction with rollability. ADA guidelines specify that accessible surfaces must be firm, stable, and slip-resistant without being so rough that they impede wheelchair movement. Asphalt naturally provides good traction, but the mix design and finishing technique directly affect whether the final surface meets this balance.
Overly coarse aggregate mixes create excessive rolling resistance for manual wheelchair users, while overly smooth finishes become dangerously slick when wet. A well-graded asphalt mix with moderate surface texture offers the best combination of grip and mobility. Proper sealcoating maintenance also plays a role; worn or oxidized surfaces lose their original texture characteristics, potentially compromising the slip resistance that wheelchair users depend on for safe navigation through parking areas and pathways.
How Should Parking Lot Layout Be Planned for Medical Facilities?
Parking lot layout for medical facilities should be planned around ADA-accessible space requirements, emergency vehicle lane placement, patient drop-off circulation, and wayfinding striping. Each element directly affects safety, compliance, and traffic flow.
How Many ADA-Accessible Spaces Are Required by Lot Size?
The number of ADA-accessible spaces required by lot size depends on the facility type and total parking count. Standard commercial lots follow a sliding scale: lots with 1–25 total spaces need one accessible space, while lots with 501–1,000 spaces need 2% of the total. Medical facilities face stricter thresholds. According to the U.S. Department of Justice, hospital outpatient facilities require 10% of patient and visitor parking to be accessible, while rehabilitation and outpatient physical therapy facilities must provide 20%.
These elevated ratios significantly impact layout geometry, requiring wider aisles, van-accessible spaces with 8-foot access aisles, and compliant slope grading across a larger portion of the lot. For a deeper breakdown of these requirements and how they affect every phase of construction, see our complete guide to planning an ADA-compliant paving project.
Where Should Emergency Vehicle Lanes Be Positioned in the Layout?
Emergency vehicle lanes should be positioned along the building perimeter, connecting directly to public roadways without requiring passage through standard parking aisles. According to the National Fire Protection Association, fire department access roads require a minimum unobstructed width of 20 feet and an unobstructed vertical clearance of 13.5 feet to ensure apparatus access.
Positioning these lanes along the facility’s primary and secondary entrances keeps ambulances and fire trucks separated from patient traffic. Designers should avoid placing parking stalls, bollards, or landscape islands within the turning radius of these lanes. For most medical campuses, a dedicated loop road around the building provides the most reliable emergency circulation path.
How Do Patient Drop-Off Zones Affect Circulation Design?
Patient drop-off zones affect circulation design by creating a secondary traffic stream that must merge safely with standard parking flow. These zones typically sit at the main entrance, requiring a dedicated pull-through lane wide enough for wheelchair loading and temporary vehicle queuing.
Effective designs separate the drop-off lane from the main drive aisle using a raised median or painted buffer. This prevents vehicles idling at the entrance from blocking through-traffic. Drop-off zones also need gentle cross-slopes for wheelchair users, which ties directly back to ADA grading requirements. For high-volume facilities, a canopy-covered loop with two exit points reduces congestion during peak hours considerably.
What Wayfinding Striping Helps Patients Navigate High-Traffic Lots?
Wayfinding striping that helps patients navigate high-traffic lots includes color-coded directional arrows, zone-labeled parking sections, and high-contrast crosswalk markings. These pavement markings guide drivers and pedestrians through complex layouts where stress and urgency are common.
Key striping elements for medical lots include:
- Blue-bordered accessible space markings with the International Symbol of Accessibility stenciled in each stall.
- White or yellow directional arrows at every decision point, such as intersections and lane merges.
- Crosswalk ladder striping at all pedestrian crossings, with stop bars set back to improve driver sight lines.
- Color-coded zone identifiers (letters, numbers, or colors) painted at row ends and repeated on signage.
Thermoplastic markings outperform standard latex paint in high-traffic areas due to greater abrasion resistance. With layout, access, and wayfinding addressed, proper drainage ensures these surfaces remain safe and functional long-term.
What Drainage Solutions Prevent Water Damage in High-Traffic Lots?
Drainage solutions that prevent water damage in high-traffic lots include proper surface grading, strategically placed catch basins, and slope design that channels runoff away from structures. Each approach addresses a specific vulnerability.
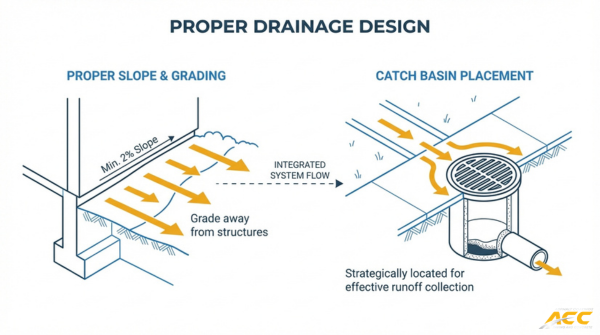
How Should Surface Grading Direct Water Away from Building Entries?
Surface grading should direct water away from building entries by establishing a consistent slope that moves runoff toward designated collection points at the lot perimeter. A minimum cross slope of 1% to 2% across the pavement surface ensures water flows predictably without pooling near doorways, ramps, or patient drop-off zones.
Grading failures at building entries create immediate liability. Water that collects near entrances seeps into foundations, erodes subgrade material beneath the pavement, and creates slip hazards on adjacent walkways. For medical facilities where wheelchair users and patients with limited mobility rely on stable surfaces, even minor ponding compromises safe access. Proper grading design starts during subgrade preparation, not as an afterthought during final paving.
Where Should Catch Basins Be Placed in High-Volume Parking Areas?
Catch basins should be placed at low points, intersections of traffic aisles, and along continuous grades where water naturally concentrates in high-volume parking areas. According to the Ohio Department of Transportation, pavement catch basins used on continuous grades are designed to intercept all flow over the grate to prevent standing water and ensure efficient drainage.
Placement priorities for high-volume lots include:
- Low points where pavement slopes converge and water collects fastest.
- Ends of long traffic aisles where runoff gains momentum.
- Near building entries and ADA-accessible routes where ponding creates the greatest safety risk.
- Adjacent to heavy-load zones like ambulance bays, where standing water accelerates pavement deterioration under repeated axle stress.
Undersizing or misplacing catch basins is one of the most common drainage mistakes in commercial lot design, often because basin locations are chosen for construction convenience rather than actual water flow patterns.
Why Is Standing Water Especially Dangerous at Medical Facilities?
Standing water is especially dangerous at medical facilities because it simultaneously threatens patient safety, pavement integrity, and emergency operations. Patients arriving by wheelchair, stretcher, or with assistive devices face heightened slip and fall risk on wet, uneven surfaces.
Beyond immediate safety concerns, standing water accelerates asphalt failure through several mechanisms:
- Water infiltrates pavement cracks and weakens the subgrade, leading to potholes under heavy ambulance and bus traffic.
- Ice formation in pooled areas during freeze-thaw cycles creates unpredictable hazards at facility entrances.
- Ponding near emergency access lanes can delay response times when vehicles must navigate flooded sections.
Facilities that operate around the clock cannot afford to close sections for emergency repairs caused by preventable water damage. With drainage strategies in place, regular maintenance keeps these protections effective.
How Do Freeze-Thaw Cycles Affect High-Traffic Facility Pavement?
Freeze-thaw cycles affect high-traffic facility pavement by driving moisture into the asphalt structure, where repeated expansion and contraction break down the mix from within. The damage compounds through cracking, chemical attack from deicers, and UV-accelerated oxidation.
What Types of Cracking Result from Freeze-Thaw Exposure?
The types of cracking that result from freeze-thaw exposure include thermal cracking, fatigue cracking, and network (alligator) cracking. Water infiltrates surface voids and expands as it freezes, generating internal pressure that fractures the binder matrix. In high-traffic zones like ambulance bays and entry lanes, heavy loads push water deeper into the pavement structure, compounding the damage with each cycle. Over time, isolated cracks interconnect into widespread patterns that compromise structural integrity. Facilities that experience dozens of freeze-thaw transitions per season face accelerated deterioration compared to standard commercial lots.
How Does Salt and Deicer Use Accelerate Pavement Deterioration?
Salt and deicer use accelerates pavement deterioration by creating rapid, repeated mini freeze-thaw cycles at the surface. Chemical deicers lower the freezing point of water, causing frequent melting and refreezing that multiplies the mechanical stress on asphalt binder. Salt solutions also penetrate micro-cracks and strip the bond between aggregate and binder, a process known as moisture damage or stripping. Medical facilities apply deicers heavily to maintain safe pedestrian access around entrances, drop-off zones, and accessible parking areas. This necessary safety practice, while protecting patients, concentrates chemical exposure in the pavement areas that already bear the highest foot and vehicle traffic.
Why Does High-Altitude Sun Exposure Increase Oxidation Damage?
High-altitude sun exposure increases oxidation damage because ultraviolet radiation intensifies significantly with elevation. According to a study published by ScienceDirect (Elsevier), UV radiation intensity at 4,000 meters is approximately 1.86 times higher than at sea level, which accelerates aging and oxidation of bituminous binders in high-altitude regions like Colorado. This oxidation hardens the asphalt binder, making it brittle and less able to flex under thermal stress or heavy loads. When combined with freeze-thaw cycling, oxidized pavement cracks faster and resists fewer load repetitions before failure. For facilities along Colorado’s Front Range, proactive sealcoating and UV-protective surface treatments are essential to counteract this compounding effect.
With environmental stressors identified, phased construction planning ensures repairs happen without disrupting facility operations.
What Phased Construction Approach Keeps Facilities Open During Paving?
A phased construction approach keeps facilities open during paving by dividing the project into sequential sections, completing one zone before moving to the next. This ensures continuous access throughout the process. Key strategies include staged paving, traffic control measures, and night paving schedules.
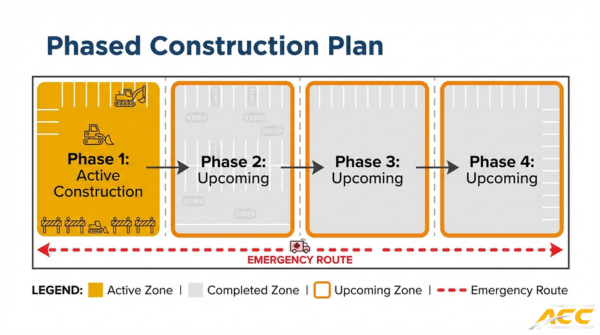
How Can Paving Be Staged to Maintain Emergency Access at All Times?
Paving can be staged to maintain emergency access at all times by isolating work to one section of the parking lot or roadway while keeping remaining areas fully operational. According to Theseus Healthcare, phased construction in healthcare facilities allows for the isolation of renovation areas to minimize noise and dust that could affect patient safety while maintaining 24/7 operations and emergency access. For medical campuses with multiple buildings, these phased paving strategies can address coordination across separate access points and tenant schedules.
Each phase is planned so that fire lanes, ambulance bays, and building entries remain unobstructed. Contractors typically work in a progression pattern, completing one zone and reopening it before closing the next. Temporary pavement markings and barriers clearly define active work zones versus open routes. For medical facilities, this sequencing requires close coordination between the paving crew and facility management to confirm that no phase blocks critical access points simultaneously.
What Traffic Control Measures Protect Patients During Construction?
Traffic control measures that protect patients during construction include:
- Temporary signage and wayfinding directing vehicles and pedestrians around active work zones.
- Flaggers or traffic control personnel stationed at key intersections to guide ambulances, patient transport vehicles, and visitor traffic safely.
- Physical barriers such as cones, barricades, and delineators separating construction equipment from pedestrian paths and vehicle lanes.
- Reduced speed zones through and adjacent to active paving areas.
- Designated temporary walkways with stable, slip-resistant surfaces for patients using wheelchairs, walkers, or other mobility devices.
Clear communication between the construction team and hospital operations staff is essential. Pre-construction meetings should establish protocols for rerouting emergency vehicles if conditions change mid-shift.
How Does Night Paving Reduce Disruption to Daytime Operations?
Night paving reduces disruption to daytime operations by shifting heavy equipment activity, noise, and lane closures to off-peak hours when patient and visitor traffic is minimal. This approach allows clinics, outpatient services, and administrative offices to operate without construction interference during business hours.
Cooler overnight temperatures can also benefit asphalt compaction in warmer months, though crews must ensure adequate lighting for quality control and worker safety. Completed sections can be opened to traffic by morning, minimizing the visible impact on daily facility operations. For facilities that never fully close, such as emergency departments, night paving still requires coordination with security and on-duty staff to maintain safe access.
With construction phasing established, a strong ongoing maintenance program keeps the new pavement performing long-term.
What Ongoing Maintenance Extends Pavement Life at Busy Facilities?
Ongoing maintenance extends pavement life at busy facilities through scheduled sealcoating, timely crack sealing, and strategic decisions about overlays versus full-depth replacement. Each approach targets a different stage of deterioration.
When Should Sealcoating Be Applied to High-Traffic Asphalt?
Sealcoating should be applied to high-traffic asphalt within the first two to three years after installation, then repeated every two to four years depending on traffic volume and environmental exposure. For medical facilities and other busy commercial lots, the high end of that frequency is often necessary because constant vehicle movement wears the protective layer faster.
Timing within the year also matters. According to the Minnesota Department of Transportation, asphalt crack sealing is most effective when performed in early spring or late fall, when cracks are open and allow better penetration and adhesion of sealant material. Sealcoating follows a similar seasonal logic; warm, dry conditions in late spring through early fall allow proper curing.
How Often Do High-Traffic Lots Need Crack Sealing?
High-traffic lots need crack sealing at least once per year, with inspections twice annually. Facilities experiencing heavy ambulance traffic, delivery vehicles, or constant patient flow should prioritize fall inspections before winter freeze-thaw cycles widen existing cracks.
Neglecting even minor cracks at busy facilities accelerates base layer failure rapidly. When damage progresses beyond crack sealing, professional commercial asphalt repair services can restore structural integrity before full-depth replacement becomes necessary. Water infiltrates through untreated cracks, saturates the subgrade, and leads to potholes that create safety hazards for patients and visitors. For any lot handling stop-and-go traffic patterns, treating cracks at the earliest visible stage is far more cost-effective than waiting for structural damage to develop.
What Triggers the Need for Overlay Versus Full-Depth Replacement?
The need for overlay versus full-depth replacement is triggered by the depth and extent of pavement distress:
- Overlay is appropriate when surface deterioration, such as minor rutting, oxidation, or shallow cracking, affects the top one to two inches but the base layer remains structurally sound.
- Full-depth replacement is necessary when base failure, subgrade saturation, or alligator cracking extends through the full pavement section.
A core sample or falling weight deflectometer test reveals whether the underlying structure can support an overlay. At high-traffic medical facilities, choosing overlay when the base has already failed only delays inevitable reconstruction at greater cost. When base integrity is confirmed, an overlay delivers renewed surface performance at roughly half the expense of full replacement.
How Should You Plan Commercial Paving for High-Traffic Facilities in Colorado?
You should plan commercial paving for high-traffic facilities in Colorado by combining thorough site evaluation with climate-adapted design. The subsections below cover how experienced crews minimize downtime and the essential takeaways for medical and high-traffic paving projects.
Can Experienced Commercial Paving Crews Reduce Downtime for Your Facility?
Yes, experienced commercial paving crews can reduce downtime for your facility by coordinating phased work schedules, maintaining emergency access throughout construction, and executing efficiently during compressed windows. Crews familiar with high-traffic environments understand how to stage equipment, manage traffic control, and sequence paving lifts so that parking areas and entry lanes remain functional.
According to the Colorado Springs Pavement Design Criteria Manual, commercial projects in the region require comprehensive field investigation and laboratory testing, including subgrade support evaluation, to ensure pavement durability in the local high-altitude climate. This level of pre-project planning prevents costly mid-construction delays.
Asphalt Coatings Company brings 39 years of Colorado Front Range experience to complex commercial projects. Asphalt Coatings Company uses in-house crews rather than subcontractors, which streamlines communication and keeps schedules tight. For facilities that cannot afford extended closures, that single-source coordination is one of the most practical advantages a property manager can secure.
What Are the Key Takeaways About Asphalt Paving for Medical and High-Traffic Facilities?
The key takeaways about asphalt paving for medical and high-traffic facilities are:
- Design for heavy loads first. Emergency vehicles impose axle weights far exceeding standard traffic, so pavement thickness, base layers, and subgrade preparation must account for these forces from the outset.
- Prioritize ADA compliance in every layout decision. Accessible parking ratios, slope limits, and surface textures are legal requirements that directly shape lot geometry and grading plans.
- Address Colorado’s climate in mix design and maintenance. Freeze-thaw cycles, intense UV exposure at altitude, and deicer use all accelerate deterioration, making specialized asphalt mixes and proactive sealcoating essential.
- Use phased construction to protect operations. Staging work in sections preserves emergency access, patient safety, and daily traffic flow throughout the project.
- Commit to preventive maintenance schedules. Crack sealing, sealcoating, and timely overlays extend pavement life and reduce long-term costs significantly. Property managers of medical facilities in southern Colorado can rely on professional sealcoating services designed for the region’s high-altitude climate and heavy traffic demands.
For facilities across Colorado’s Front Range, partnering with a contractor that understands these intersecting demands makes the difference between reactive repairs and lasting infrastructure.